
A Guide to Rapid Triage
23rd April 2018
Triage is the process of sorting casualties in order of priority which sounds simple enough, unfortunately without an understanding of how to effectively, objectively and accurately do this we have a habit of making these decision based on the wrong criteria: We follow common heuristics such as ‘going for the quiet ones’ or ‘treat unconscious casualties before conscious casualties’. Humans are also genetically hardwired to react to the sight of blood so we triage based on injuries; treating the most visibly traumatic – the blood guts and gore – over less obvious injuries.
This is wrong.
- Casualties are not triaged based on how loud or quiet they are.
Someone emotionally traumatised may be laying foetal in the corner not saying a word, someone with a femoral bleed may be screaming in agony.
- Casualties are not triaged based on whether they are consciousness conscious or not.
A casualty can be unconscious but otherwise perfectly healthy (feinting) or they could be fully conscious but expected to deteriorate and die very quickly.
- Casualties are not triaged based on their injury
Injuries do not necessarily tell you if a casualty is going to die. The vital signs do. A bleeding head wound can look horrific, even though it is essentially superficial. A sucking chest wound or internal head injury can kill a casualty quickly…without producing that much blood.
So if all of these standard rules we have either been taught or assumed are unfounded, how do we prioritise casualties?
The Triage Process
There are many algorithms used to quickly triage casualties utilised by UK, US and other international healthcare professions. They are tried, tested and effective but complex; even a seasoned veteran would be expected to resort to their Aide Memoire or Crib Sheet on arrival at a major incident.
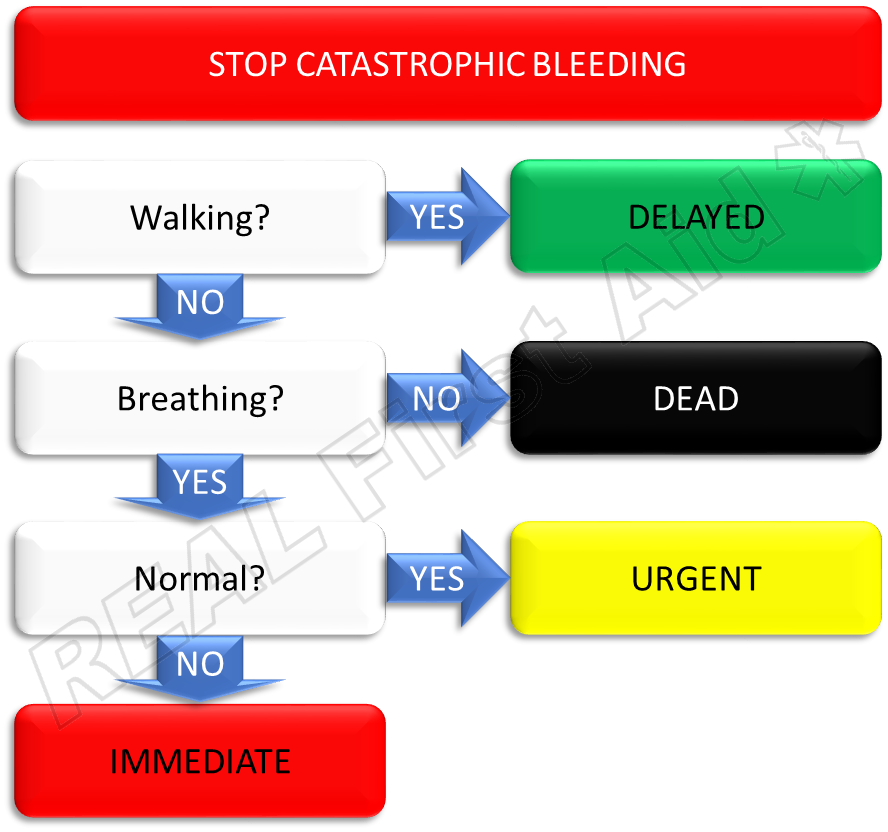
For the First Aider we promote a distilled version; it is simplified making it easier to remember and apply but works through the same robust mechanism:
Are they Walking?
Are they Breathing?
Is it Normal?
1. Are they walking?
Anyone who is walking around has either the mental capacity or physical ability to mobilise themselves. They are by the nature of their abilities less serious than some who is not able to do so.
These people are your walking wounded. Utilise them or direct them away from the incident to help.
These are Category 3 casualties – Delayed
2. Are they breathing?
If the casualty appears unconscious, properly check the mouth and clear it if necessary, then open they airway by tilting the head (forget about spinal injuries right now….if you don’t have an open airway you don’t have a casualty).
If you are confident they are not breathing, they are are Category 0 casualties – Dead.
(Ordinarily, with a single casualty, we would now summon a defibrillator, call the Emergency Services and commence CPR. In a multi-casualty scenario, dead people are not casualties. Help those who are still alive.)
3. Is it normal?
If they are breathing, is it normal?
If they are on the ground they are in a more serious condition than those who can’t walk so they are a higher priority than a Category 3 Delayed.
If they are breathing normally they are Category 2 casualties – Urgent.
If they are not breathing normally they are Category 1 casualties – Immediate.
How someone breathes is one of the most revealing indicators of their state of health but forget about clinical metrics; quite simply does their breathing seem normal? Normal speed, effort and depth? Normal breathing is slow, easy, regular and silent - any change to this indicates a problem.
- Noisy breathing can indicate an airway problem
- Slow, deep heavy breathing can point to a head injury
- Fast, weak breathing when someone is cold and pale indicates blood loss
All of these life threatening conditions can be present regardless of whether there is a visible injury and regardless of whether they are conscious or not.
How to Triage
It is vitally important that the Triage process does not involve treatment (with three exceptions explained below). It is far too easy to get drawn into dealing with the first casualty you come across…at the expense of other casualties.
Triage is an objective, emotionless process. Almost ruthless. This is fundamental to allow us to administer the best care to as many casualties as possible rather than to the few at the expense of the many.
Step 1: Take charge – poor communication leads to casualties being missed or triaged twice.
Step 2: Triage everyone – use Bystanders and the Category 3 casualties to sit with or tend to Category 1 and 2 casualties as you identify them.
Step 3: Identify all of the Category 1 casualties. These are where your priorities are and where we direct our time and resources. When the emergency Services arrive, direct them to these casualties first.
Step 4: After you have stabilised the Category 1 casualties DO NOT move onto Category 2 casualties – things change so triage everyone again. Category 3 casualties deteriorate and become Category 2, category 2 casualties become Category 1 and some Category 1 casualties will become Category 0.
Exceptions
As a rule we do not get involved in any treatment while we are triaging but there are three interventions we apply as we triage:
- Unconsciousness:
Place all unconscious casualties on their front before you move on. If they are unconscious but breathing normally they are category 2. If you leave them on their back with will very quickly become Category 0 because you failed to protect their airway.
- Catastrophic haemorrhage:
A catastrophic haemorrhage can be defined as an ‘immediately life threatening bleed’ – this is an arterial bleed which is actively pumping.
If blood is squirting out of a casualty a) they still have lots of blood and b) their heart is working well. If blood isn’t actively pumping out, if it has just pooled and not getting any bigger, ignore it - either it isn’t catastrophic (and therefore not time critical) or they are dead.
Stop the bleeding with a tourniquet (dedicated or improvised) if it is on a limb or wound packing if it is abdominal.
- Injuries incompatible with life
Some injuries are not compatible with life, regardless of how prompt or effective their treatment. In a multiple casualty situation we do not get involved with treatment for these casualties as it diverts resources from seriously injured casualties who are more likely to survive if they receive prompt, effective treatment. These situations are:
- Decapitation
- Massive cranial and cerebral disruption
- Hemicorporectomy (torso separated in half) or similar massive injury
- Incineration (>95% full thickness burns)
- Decomposition
- Rigor mortis (rigidity of the body) and hypostasis ( a discolouration of the body where blood pools to the lower half as blue mottling underneath the casualty, evidence of death after a number of hours)
Triage Exercise
Triage each of these casualties into either Immediate, Urgent, Delayed or Dead.
- A teenage boy is limping, he tells you he has a broken ankle.
- The driver, a 38 year old male is slumped over the steering wheel, unresponsive and not breathing.
- A middle aged female is unconscious but breathing fast ( > 25 breaths per minute)
- An unresponsive male appears to be snoring. His breathing improves when you open his airway.
- An elderly casualty is found, disoriented on the floor but breathing normally.
- A middle aged male is found, unable to move is clearly injured legs but is breathing normally.
- A 57-year-old female is conscious with no obvious injuries but breathing fast. She is cold and pale.
- An young child is found unresponsive and not breathing.
- A young woman approaches you and offers help
- A middle aged male with an obvious head injury and exposed brain tissue.
Answers
Highlight this text and drag downwards to reveal the hidden answers.
- A teenage boy is limping nursing a broken ankle.
Delayed – The casualty is walking so we assume the have normal mental capacity (not indicative of a head injury) and they are no seriously injured).
- The driver, a 38 year old male is slumped over the steering wheel, unresponsive and not breathing.
Dead – in a multiple casualty situation, resuscitation is not appropriate.
- A middle aged female is unconscious but breathing fast ( > 25 breaths per minute)
Immediate – The fast breathing indicates shock. The fact that she is unconscious is not a triage factor.
- An unresponsive male appears to be snoring. His breathing improves when you open his airway.
Immediate – The snoring indicates either a compromised airway or a head injury. The fact that he is unconscious is not a triage factor.
- An elderly casualty is found, disoriented on the floor but breathing normally.
Urgent – The casualty is unable to walk which indicates he is more seriously injured that someone who can (Delayed), but his breathing is normal so he is not as serious as others (immediate). His age is not a triage factor.
- 2 A middle aged male is found, unable to move is clearly injured legs but is breathing normally.
Urgent – The casualty is unable to walk which indicates he is more seriously injured that someone who can (Delayed), but his breathing is normal so he is not as serious as others (immediate). Neither his age, nor obvious injuries are triage factors.
- A 57-year-old female is conscious with no obvious injuries but breathing fast. She is cold and pale.
Immediate – The fast breathing and pale skin indicates shock. The fact that she is conscious compared to #3 is not a triage factor.
- An young child is found unresponsive and not breathing.
Dead – despite their age, in a multiple casualty situation, resuscitation is not appropriate.
- A young woman approaches you and offers help.
Delayed – The casualty is walking so we assume the have normal mental capacity (not indicative of a head injury) and they are no seriously injured).
- A middle aged male with an obvious head injury and exposed brain tissue.
Dead – without needing to check breathing the casualty has an injury which is not compatible with life.
Highlight this text and drag the cursor upwards to reveal the answers.